


Health Update & a Request for Collaborative Ripple Effects
Many of you have asked for an update on my health.
And many of you have watched me navigate these mountains over the years. I’ve always tried to be transparent about what I’m facing — so first, thank you. Your messages and care mean more than you know.
That said, simply giving an update about “me” feels out of alignment with why I have social media or built Operation Human First in the first place.
Operation Human First was never meant to center my story. It was built to help other humans suffer less and improve their health.
So instead of sharing this as a personal update, I’m sharing it as a catalyst and asking you to be a part of the change.
What I’ve experienced — while unfortunate — is not unique. I can almost guarantee that someone you know right now, or someone you will meet in your lifetime, is navigating one of these same conditions.
While one of my conditions is extremely rare, the other is not. Rather, it is simply extremely poorly understood and under diagnosed.
If this “update” does anything, I hope it creates a ripple effect.
If you’re in healthcare — physician, nurse, physiotherapist, manual therapist, or otherwise — I ask you to read what follows with curiosity. Question assumptions. Seek updated education. Consider how these patterns might show up in your patients.
I’m doing the same.
Because the body is not a collection of isolated parts. It is an integrated system. And when we treat it through a narrow, reductionist lens — assuming a condition tied to one organ cannot influence others — we miss the bigger picture. Sometimes at great cost
Let’s do better. Together.
Connecting the Dots in a Lagging System
For over 15 years, I lived with escalating symptoms. In that time, I saw:
14 specialists
5 family doctors
Countless ER physicians
2 Functional medicine practitioners
3 Naturopathic doctors
Not one was able to connect the dots.
This isn't a story about bad doctors. Most were skilled, well-intentioned, and genuinely wanted to help. It's a story about a system built on specialization, where the space between specialties becomes a blind spot – and patients like me fall through it.
Many of you have followed my journey since I traveled to the United States one year ago to learn more about the autonomic nervous system through courses with the Postural Restoration Institute. That trip marked the beginning of my neuro-rehabilitation journey.
For the first time, significant pieces began to make sense.
We uncovered unresolved effects from multiple traumatic brain injuries, including:
Impaired visual processing
Vestibular dysfunction
Trauma-induced instability in upper cervical joints (the joints that hold the skull on the neck, in close proximity to the brainstem)
Each of these issues was anchoring my system in chronic sympathetic activation — a sustained “fight or flight” state.
I was prescribed what I call my “neuro-glasses” (“glasses for my brain, not my eyes”) and a mandibular orthotic (a sensory stabilization tool for my neck and nervous system).
I began retraining how my brain processed sensory input. The change in my spine range of motion was immediate.
For the first time, I experienced relief that made neurological sense.
However, I could also tell that something else was still flying under the radar.
Despite improved movement, the following persisted:
Altered blood sugar responses
Hormonal abnormalities (subtle on bloodwork but obvious to me and on both saliva/urine testing)
Exaggerated immune and inflammatory reactions
GI symptoms that resembled obstruction and did not respond to diet
Cyclical pelvic, abdominal, and joint flare-ups
Recurrent hemorrhagic cysts
Significant peritoneal pain after cyst rupture
Daily hiccups and diaphragm spasms that flared alongside everything else
The nervous system explanation was real — but it wasn’t the whole story.
Then, after eating wagyu steak for the first time in Bali in between cyst ruptures — everything escalated.
My symptoms were no longer manageable.
Research & Detective Work
I wasn't getting any answers, so I decided to take my health into my own hands by:
Making a list of all my symptoms over the years, in the order in which they started.
Writing down all of my observations about my body, which were not necessarily symptoms but things I knew both logically and intuitively were not normal.
Reviewing 1.5 decades worth of my blood work & labs, all organized into a spreadsheet where I could see patterns.
Reviewing every single radiological report, biopsy report, colonoscopy/endoscopy report, gastric emptying study, functional medicine hormone report, and microbiome study I've ever had done.
Eventually I came across the condition that the advanced ultrasound mapping in London would later confirm that I have.
The first thing you need to know about this condition is how it behaves, so you can recognize it as it is frequently missed.
Misunderstood Pathophysiology
Once I really started investigating, I realized something unsettling: myself and every practitioner I'd ever worked with had all misunderstood this condition. Here's what we all missed:
It's systemic, not local.
While benign, it behaves almost like cancer – invading tissues, developing its own blood supply, resisting cell death.
It can spread physically to areas you wouldn't expect: the brain, diaphragm, joints, lungs.
It impacts immune function, metabolism/insulin, digestion, hormones, and the nervous system.
It can now be diagnosed with advanced ultrasound by trained specialists
Research also shows many cases have:
Reduced natural killer (NK) cell activity
Overactive inflammatory immune cells
Elevated inflammatory cytokines
Altered macrophage behavior
Further, the immune cells fail to recognize abnormal tissue or lesions.
This gives abnormal lesions a chance to “fly under the radar” as the body thinks they are normal.
These abnormal lesions can then develop and thrive in the abdominal cavity.
Meanwhile, these lesions have a higher numbers of activated mast cells within them, which dump the following into the abdominal cavity:
Histamine
TNF-α
Other inflammatory mediators
The Brain Injury & Neurological Connection
We know with certainty that the 14 instances of traumatic brain injuries and decades of unresolved sensory issues following kept me in a state of autonomic nervous system dysfunction and sympathetic dominance (a chronic state of physiological “fight or flight”).
What I did not know until recently is that this coincidentally creates/contributes to a perfect internal environment where lesions in this condition can develop and thrive.
This is not specific to brain injuries. Rather, anything that contributes to autonomic nervous system dysfunction can also play a role in this condition.
Misinformed Medical Recommendations
Following learning all of this, I ended up in the emergency room after having my second hemorrhagic cyst rupture.
This resulted in abdominal muscles that were very painful when upright, coughing, etc., along with lab findings showing an inflamed bladder (no UTI) alongside my existing inflamed GI tract from Bali. I had a large apprehensive bubble that felt “unstable” in my abdomen, nausea, and a bowel that felt blocked under my left ribs.
They did a CT scan with contrast and two ultrasounds, all confirming another hemorrhagic cyst rupture.
Beyond that? Nothing. They assured me the cyst would heal on its own over a few months.
When I mentioned the condition I was planning to investigate in London, they dismissed it as "a far reach” and stated that diagnosis can only be done with surgery.
Two days before flying to London, a gastroenterologist reiterated the same advice: unlikely, unnecessary, don't bother.
SMAS Syndrome & Nut Cracker Awareness
Before I dive into what the imaging in London revealed, I’ll explain what my hospital CT scan did catch – even though it was overlooked at the time.
The radiologist noted that I have a lack of mesenteric fat. For most people, this is an incidental finding, insignificant. For me, it explained why I crashed after eating wagyu in Bali.
Years earlier, a specialist realized I have all of the symptoms of Superior Mesenteric Artery (SMA) Syndrome and Nutcracker Syndrome – rare anatomical variants where the angle between the aorta and superior mesenteric artery is too narrow.
This causes compression of the small intestine and left kidney vein as they pass through that space. The lack of mesenteric fat means there's no cushion protecting them.
My symptoms dated back to age 8 (abnormal urine at my first checkup), but it took until I was nearly 30 to get the anatomical confirmation. The photo below is a photo I took where my hepatobiliary and pancreatic specialist was showing me my narrow angle.
What this looks like day to day:
SMAS primarily affects digestion:
Early satiety (full after a few bites)
Delayed gastric emptying with visible upper abdominal swelling (worse with fatty or fibrous meals)
Nausea, distension, extreme post-meal pressure
Spikes of post-meal sympathetic nervous system activity that's actually vagus nerve irritation (not psychological)
Nutcracker affects kidneys and vascular flow:
Blood or protein in urine
Left flank pain, pelvic pressure
Orthostatic intolerance, fatigue, dizziness
Symptoms often flare with menstruation
The overlap is significant – and so is the clinical catch-22.
If I get too lean, my symptoms worsen because there's even less cushion.
But after my cyst ruptures, I'd been trying to lean out because of the rapid "weight gain" around my lower abdomen. I didn't yet know that gain was inflammation from the undiagnosed condition I’d later find out I had in London.
For the clinicians reading: living with these conditions as a physical therapist has given me a front-row seat to how they affect the body.
It impacts the diaphragm, spine, rib flare (especially left, with downstream consequences for the shoulder), the autonomic nervous system, intra-abdominal pressure regulation, etc.
This is why generic exercise programs fail certain people. If someone isn't responding, it's worth asking: is there an anatomical or medical reason they can't?

Advanced Imaging for Diagnosis in Europe
I ultimately decided to ignore the noise, follow my instincts, and fly to the United Kingdom to pursue the advanced ultrasound mapping.
Using the advanced ultrasound, the specialist was able to find:
Numerous deep infiltrating lesions
A map of which organs were involved in the lower abdominal/pelvic cavity
Tethering and compression of my bowel
Areas around my bowel/organs that the report states are “partially obliterated with adhesions”
They also explained to me that the hemorrhagic cysts that I’d been seeing on ultrasound in Canada and had been struggling with since September are a common feature of this condition, which was not the information that I got in Canada.
These cysts are often written off as “normal”, when they are not.
They also explained that my system and hormones finally improving – a win from my year of neuro-rehabilitation – had an unexpected downside: my ovaries "came back online."
Ovulation starting up again triggered hemorrhagic cysts that rupture repeatedly. This hadn't happened sooner because my ovaries had been "asleep" while I was combatting post-concussion HPA axis dysfunction.
Further, that when these cysts rupture like they had been, the associated bleeding in the abdominal cavity can “pour gasoline on the fire of lesions” causing a cascade of inflammation, pain, and hormone responses.
Through my own research, I’ve also learned that the hormonal landscape that my brain injuries left me with is also the same hormonal landscape that tends to breed this condition.
My progesterone tanking after my brain injuries and staying chronically low while my estrogen was “running wild and free/unopposed”, may have been a contributing or complicating factor.
I need to do more research on all of this yet.
This is simply my understanding of the information I have been given so far and based on the limited time I’ve had to investigate this since I sat down to try to figure all of this out weeks ago.
I will continue to do more reading to try to understand the global systemic picture, and I have reached out for professional insights where I can.
As I learn more, I will share more for anyone else that it can help.
I have held off on naming this multi-system condition until this point as I first wanted to create a picture of what it “actually” is before I gave it the label that is typically associated with wildly outdated information. For example, many people still think it is:
“A local” condition (false)
Gynaecological or pelvic condition (false)
“Menstrual cycle-specific” condition (false)
Disease that can only be diagnosed with laparoscopy (false)
The condition I'm describing and was diagnosed with is a sub-type of endometriosis called deep infiltrating endometriosis (DIE).
The volume of outdated, false information still being circulated about endometriosis isn't just frustrating – it's harming people. It leaves them:
Unable to get diagnosed at all
Believing surgery is the only way to even find out if they have it
Making treatment decisions without full information
This has to change.
My hope is that the information that I put here helps:
Improve awareness of options actual and diagnosis and treatment options available.
Improve timelines while reducing suffering for those with this condition.
Reduce the number of people who are misinformed about it (which I'll be first to admit was me only a few weeks ago).
Practitioners/clinicians, please also know that endometriosis can show up joints and tissues. In a systematic review of reported cases of musculoskeletal endometriosis, lesions were described in sites such as:
Abdominal muscles (50.7%)
Pelvic floor muscles (11.6%)
Lower limb muscles (11.6%)
Hip muscles (8.7%)
Lumbar muscles (7.2%)
Joints (5.8%) — I’ve clinically seen one client who has it in her knees since learning this.
Upper limb muscles (2.9%)
Shoulder–neck muscles (1.4%)
You can read more in this systematic review.
If you consider the pathophysiology of what happens in lesion locations (above), you’ll see that this is clinically significant.
Additional Clinical Insights Gathered Through Ultrasound
Here are some additional insights that I gathered from my appointment in London that could be of use to women and practitioners:
They didn’t just see the deep infiltrating lesions.
They showed me that certain organs were not moving when probed with the ultrasound.
Healthy pelvic organs glide and move relative to each other.
For my manual therapists out there, this is similar to how we should see layers of tissue move relative to one another.
My organs do not move when probed or pushed on. They are “stuck”.
My intestine is also stuck and tethered.
They also made a point of going through, pushing on lesions, areas of tethering, and so on to find and map exactly what causes certain symptoms/pain that I’ve had.
That process explained something I had lived with for years:
For many years (especially when I had my “mysterious” microscopic lymphocytic colitis), I woke up every morning to unrelenting left-sided abdominal pain. This pain came back with a vengeance after my first and second hemorrhagic cyst ruptures in recent months.
They were able to “see” what I had “felt”, replicate my pain by prodding the area of my bowel that is tethered, and point out exactly what was causing it (and show me on the live feed).
Seeing that my bowel was tethered in place and that the surrounding area was “partially obliterated with adhesions” (according to the report), reframed years of symptoms that nobody else in the last 15 years was able to explain.
The Europe Shortcut
For anyone wondering or considering this route, I had my exam done at:
Gynecology & Ultrasound Centre, 137 Harley Street, London (UK)
Cost of the exam + consultation: ~$950 CAD (excluding flight & accomodation costs)
Results: They gave me my results in real time as the specialist did the exam himself and explained exactly what he was seeing and showed me everything as he did the exam. He then proceeded to sit with me afterwards to answer any questions that I had — and I had many.
My appointment was at 9am London time on Monday, and I had the results with a full 5 page report/letter to my doctor in my inbox along with the images from the ultrasound by the time that I woke up Tuesday morning in Canada.
Finding & Advocating for Advanced Ultrasound Mapping
Since returning, I have been actively investigating whether advanced endometriosis ultrasound mapping is available in Canada — and if not widely available, who may be pursuing it (while actively trying to encourage specialists to pursue it).
Several centers/specialists I’ve spoken with are not currently offering structured endometriosis-specific mapping.
However, some have been open to learning more about the evolving literature and diagnostic approaches. That gives me hope.
Advanced sonographic mapping of endometriosis is not a routine pelvic ultrasound. It requires:
Specialized training in endometriosis imaging
A structured, endometriosis-specific protocol
Assessment of organ mobility (e.g., sliding sign)
Evaluation of deep structures including bowel and uterosacral ligaments
In some centers, pain mapping during the scan
This approach has been formalized internationally through the IDEA consensus (International Deep Endometriosis Analysis group) and subsequent imaging consensus updates.
For deep infiltrating endometriosis (DIE), expert transvaginal ultrasound can detect disease with high specificity and can assist in surgical planning. MRI is also used in many centers.
Importantly:
Deep infiltrating endometriosis and endometriomas can often be diagnosed accurately through expert imaging, and surgical confirmation is not always required before initiating treatment.
In my case, the only diagnostic option offered locally was laparoscopy. Based on what I later learned, this would have confirmed disease but would not have fully addressed the complexity of my deep infiltrating lesions.
Specialists in London advised that surgery for my level of DIE should be performed exclusively by a surgeon with advanced excision training, often within a multidisciplinary team when bowel or diaphragmatic involvement is suspected.
This distinction matters. Surgical outcomes for complex DIE are closely linked to surgeon expertise and case volume.
Had I undergone a routine diagnostic laparoscopy first, I would have required a second surgery for definitive excision. This would have been two large inflammatory events, which has implications in any body and even more so for those with an inflammatory condition.
Advanced imaging helped clarify the surgical complexity beforehand and further imaging (MRI) is needed to continue mapping the lesions.
Current Canadian Investigation
One center that lists specialized imaging alongside MRI is:
BC Women's Hospital and Health Centre
When I contacted them they communicated:
They perform pelvic ultrasound
They assess bowel involvement
They perform pain mapping'
Referrals typically come from a family doctor or gynecologist
Patients usually have trialed at least one first-line therapy
They primarily see BC and Yukon residents
They were unable to confirm whether their protocol mirrors the exact technique used in London for structured DIE mapping, but it sounds like it may be in a similar domain.
I am continuing to investigate options locally and in other provinces and will update this page as I learn more.
Ontario is currently offering a fellowship program that covers the advanced ultrasound procedure I had done in the United Kingdom, so once again I am optimistic.
Why This Matters
Endometriosis has historically been thought to require surgical confirmation for diagnosis. That model is finally evolving.
Expert imaging can now:
Reduce unnecessary surgeries
Help stratify surgical complexity
Guide referral to appropriately trained surgeons
Allow better pre-operative counseling
Reduce repeat surgeries
As awareness increases, my hope is that more Canadian clinicians pursue training in advanced endometriosis imaging and that referral pathways become clearer and more accessible.
Until then, I will continue sharing what I learn.
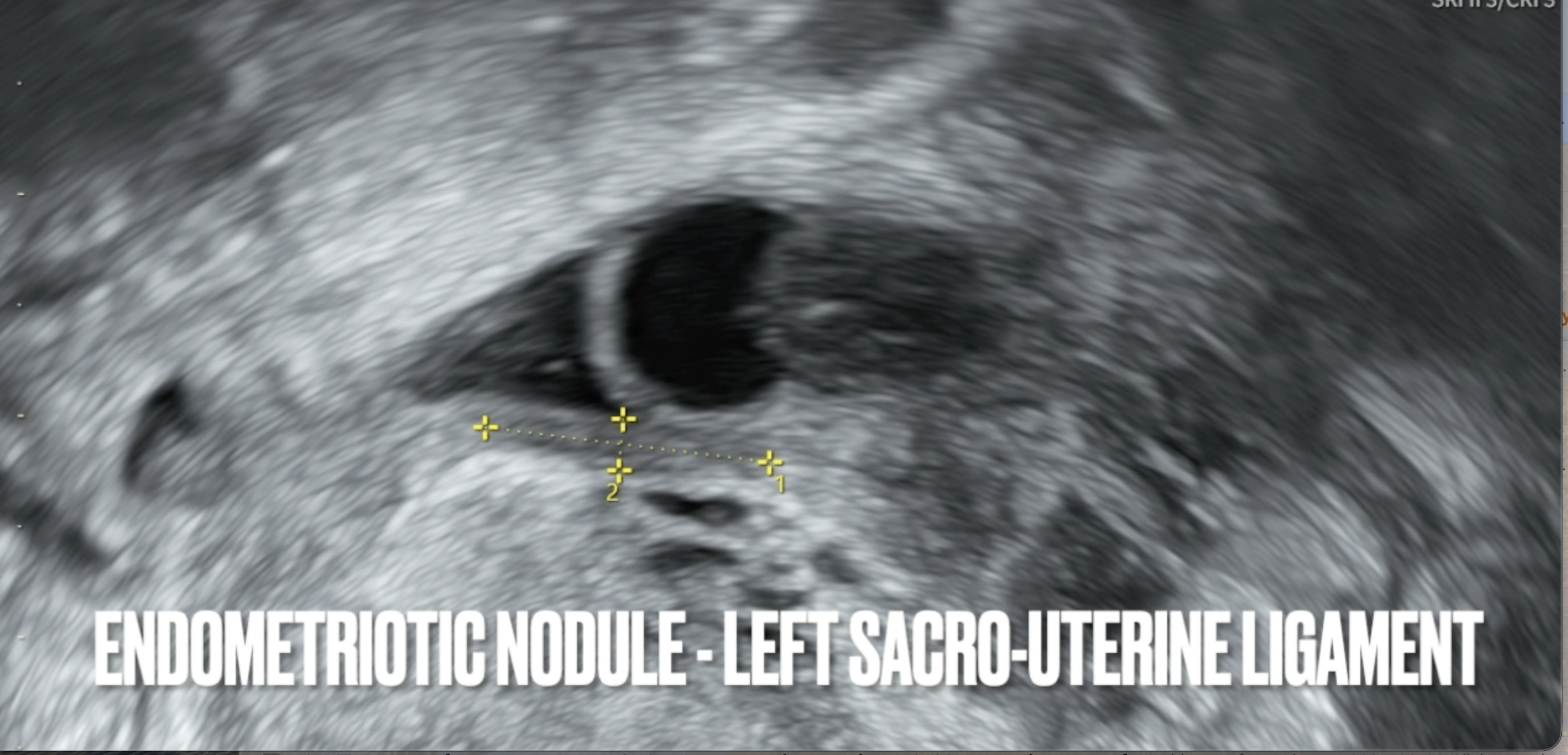
The specialist in London was kind enough to record the entire scan for me, label it, and send it to me - which I’ve offered to share with local specialists interested in learning more.
Here is a screenshot demonstrating how you can see, measure, and diagnose deep infiltrating endometriosis on ultrasound.
Thanks to them, I now have an objective way of seeing if the lesions are worsening/improving.
Visceral Insights Gained Through Advanced Sonography
Years ago, during my microscopic colitis nightmare, I saw a pelvic floor therapist in Saskatoon who offered visceral manipulation.
She did an exam. Found some subtle pelvic floor tightness – nothing extreme, proportionate to the inflammation I was carrying.
Then she did visceral work and said something strange:
"Your descending colon feels stuck."
I didn't know what that meant. Didn't have the diagnosis yet. Didn't even really understand what visceral manipulation was.
But now? I realize that was a clue. Information I could have taken back to my doctor and pushed further with.
So if you're stuck in the diagnostic void, waiting for imaging that's hard to access: know this:
Skilled pelvic health practitioners and visceral therapists may detect movement restrictions that are consistent with adhesions in endometriosis.
It's not a diagnosis. But it's information. And information is what builds a case.
Accessing Visceral Practitioners
I've reached out to the pelvic floor & visceral clinician that saw me for that appointment as well as another practitioner. Pending their permission, I will include their contact information here (check back later).
I will also be having conversations to see if I can find practitioners who are willing to write supportive letters outlining any pelvic floor or visceral restriction findings that could be consistent with endometriosis, to see if this helps speed referral pathways.
I also know many of you that follow me on Instagram or are clients of mine are also physicians. If you have any insight on information that we could include that might help with this referral pathway, I am also all ears and happy to include it here.
If it helps even one human move faster, it’s worth attempting.
New Diagnostic Options
Non-Invasive EndoSure Test
Days before I went to London, I saw a client of mine who is a family physician in Saskatchewan. She informed me that she had a patient who had received a positive diagnosis of endometriosis by getting an ENDOSURE test done, which came back positive for endometriosis.
She was very transparent and admitted that she had never heard of the test before and still did not know much about it, however she did recognize it as a positive result. Further, based on the test results and her patient’s symptoms, she made a referral to a endometriosis excision specialist here in Saskatoon. She also informed me that the specialist accepted this as a positive test result and thus accepted the referral as well.
I have contacted that specialist regarding this test as well as the advanced ultrasound and their staff has told me that the surgeon or a staff member will look into both and reach out. I am currently waiting to hear back.
According to their website “The ENDOSURE test uses an electroviscerography system (EVG), an analytical instrument that collects Gastro Intestinal Myoelectrical Activity (GIMA) signals from the abdomen through dry electrodes.”
There was a test available in Calgary at Frami Chiropractic until September 14th but is currently paused while the clinic assesses the business model to see if fits into their practice.
If you are in Alberta or Western Canada and want this test brought back to Calgary, I strongly recommend contacting the clinic and asking to be placed on a waitlist.
Interest drives availability.
In the meantime, it looks like it is offered in Edmonton as well as in Ontario (shown here). I've reached out to clinics in both, or to both clinics about 4-5 times each now; unfortunately, I have yet to get a response back.
My (current) understanding:
It can indicate whether endometriosis may be present.
It does not tell you where it is.
I cannot say that every physician or specialist will accept this test or the results. This is not currently considered a definitive diagnostic test in major guidelines, and acceptance may vary widely by clinician and province.
I can only say that some physicians are using this to support referrals. According to the reception staff at the BC Women’s Hospital & Health Center, while they were unfamiliar with this test they did state that they would accept it with a family doctor’s referral letter as well.
If you are simply trying to get an answer on if you have endometriosis or not so you can start taking steps forward, you might find it of use to you as well.
Magnetic Resonance Imaging (MRI)
It seems to be that the most up-to-date surgical centers are using a combination of advanced ultrasound as well as MRI for pre-operative assessment.
From what I understand so far, MRI is useful for:
Mapping deep infiltrating disease
Bowel involvement
Diaphragmatic involvement
But it must be ordered correctly and read correctly.
If you are a radiologist, surgeon, or are familiar with proper MRI protocols for endometriosis in Canada, I welcome and appreciate your input!
This section will be updated as I learn more.
Surgery Decision Making
I truly have so much more reading to do to understand this condition as a whole, as well as to understand what surgery can and cannot offer.
To date I've been told that the only treatment options are:
Inducing menopause
Hormonal birth control to stop getting a period
Excision surgery
However, it is not lost on me that the same people that I'm hearing that from were also the same people that did not recognize this condition and/or were providing me with outdated information earlier.
As such, I do not subscribe to the belief that these recommendations are the only options or that surgery will somehow fix a multi-system condition condition like this.
My Current Logic
I do not believe that it makes sense for me to jump to surgery when I don't yet have all of the answers on exactly where the endometriosis is within my body.
My presentation suggests that deep infiltrating lesions in my upper abdomen or within my diaphragm should be assessed.
If this is present, I would need a different surgical team than I would if it is only present in my lower abdominal cavity or pelvis.
I personally will be advocating that I not be sent for surgery until we know exactly which surgeons are needed on my team (and until I have researched each surgeon).
Further, the SMAS/Nut Cracker Syndrome adds a layer of complexity that needs to be closely considered. Especially if I might need a diaphragm resection.
There is a lot to be considered overall.
For now, the question right now is not:
Do I get surgery or not?
Rather, for me, the question right now is:
How does somebody in Canada access the type of MRI & protocol needed in order to finish mapping these lesions and investigate their presence in the upper abdomen or diaphragm.
Once again, I welcome any and all information and resources on this.
This is not a question that I am working to solve for my case alone — as women everywhere need these answers and pathways.
Specialists internationally that are leading the way in this condition are developing a standard of performing advanced ultrasound and MRI pre-operatively.
However, in Canada, accessing this standard of care currently appears to require significant detective work and advocacy.
As I work to figure that out, I am simply trying to better understand:
The pathophysiology of DIE.
It’s systemic nature and the autonomic nervous system overlap.
Exactly what that internal environment this disease thrives in.
How I can also work on inducing positive adaptation to improve that environment in such a way that inhibits this condition from thriving.
I can only assume that doing so will:
Give me an idea of how much I can improve my health conservatively while I wait/try to navigate our system to finish mapping the condition.
Set me up for a better result & recovery if I do need surgery.
Improve the odds of a successful recovery post-surgically.
For Self-Advocating Patients & Open Minded Clinicians
I know not everyone has training in reading scientific literature. It can feel like a foreign language.
So I've put together a brief list of peer-reviewed articles below, along with key takeaways from each – digestible enough to bring to your doctor, rigorous enough to be taken seriously.
If you're a clinician reading this and want to learn more: thank you. You're exactly who this ripple effect needs.
Where I Can Improve as a Practitioner
Surgical Incision Considerations
While digesting all of this, I've had to reflect on my own role as a practitioner. There's one area I know I can improve immediately – and I owe it to a past client to name it publicly.
He came to me after an organ donation, struggling with his surgical incision. (He's also the one who started the rubber duck trend in my clinic – the one OHF subscribers won't let me forget.)
I explained to him how surgical incisions affect the layers of tissue – how they need to slide and glide relative to each other for proper nerve function, circulation, healing. We worked on his scar. His symptoms resolved.
Then he asked me something I'll never forget: "Can you help other post-operative patients learn about this?"
I wrote a few letters for him to assist him in trying to improve awareness around this within organ donor communities and organizations.
However, I also told him that I would try to do a better job of informing people that this is something to consider post-surgically and that this is also something that I treat myself if anyone ever needs.
I told him I would. Those rubber ducks? In retrospect, each one should have been a reminder.
If there is anyone locally that is recovering from a laparoscopy or surgery and needs treatment, please feel free to contact me. Regardless of if I am booking months in advance.
I will do what I can to set aside time to serve this population better than I have.
If you ever find yourself needing surgery, I hope the bit of information above is helpful to you.
That is all I have for now, I’ll update this as I can/when I can, and as I learn more.
With gratitude,
Alex
Have information or resources to contribute?
To contribute any information or resources or if you have any insight on pathways available in Canada, please contact me via email. And, THANK YOU for doing so.
For general conversations, please message me on Instagram.
Disclaimer: The content shared here represents my personal health journey, my own research, and my current understanding of the conditions I'm navigating. I am a physical therapist, but I am not a physician, and I am not your healthcare provider.
This information is for educational and informational purposes only. It is not medical advice, diagnosis, or treatment. Never disregard professional medical advice or delay seeking it because of something you've read here.
Medical knowledge evolves, and my understanding will continue to develop. I've done my best to ensure accuracy, but I may not be aware of every update in the literature. You should consult qualified healthcare professionals who know your unique situation before making any decisions about your health.
If you're experiencing symptoms, please seek appropriate medical care. If you're in crisis, contact emergency services in your area.